




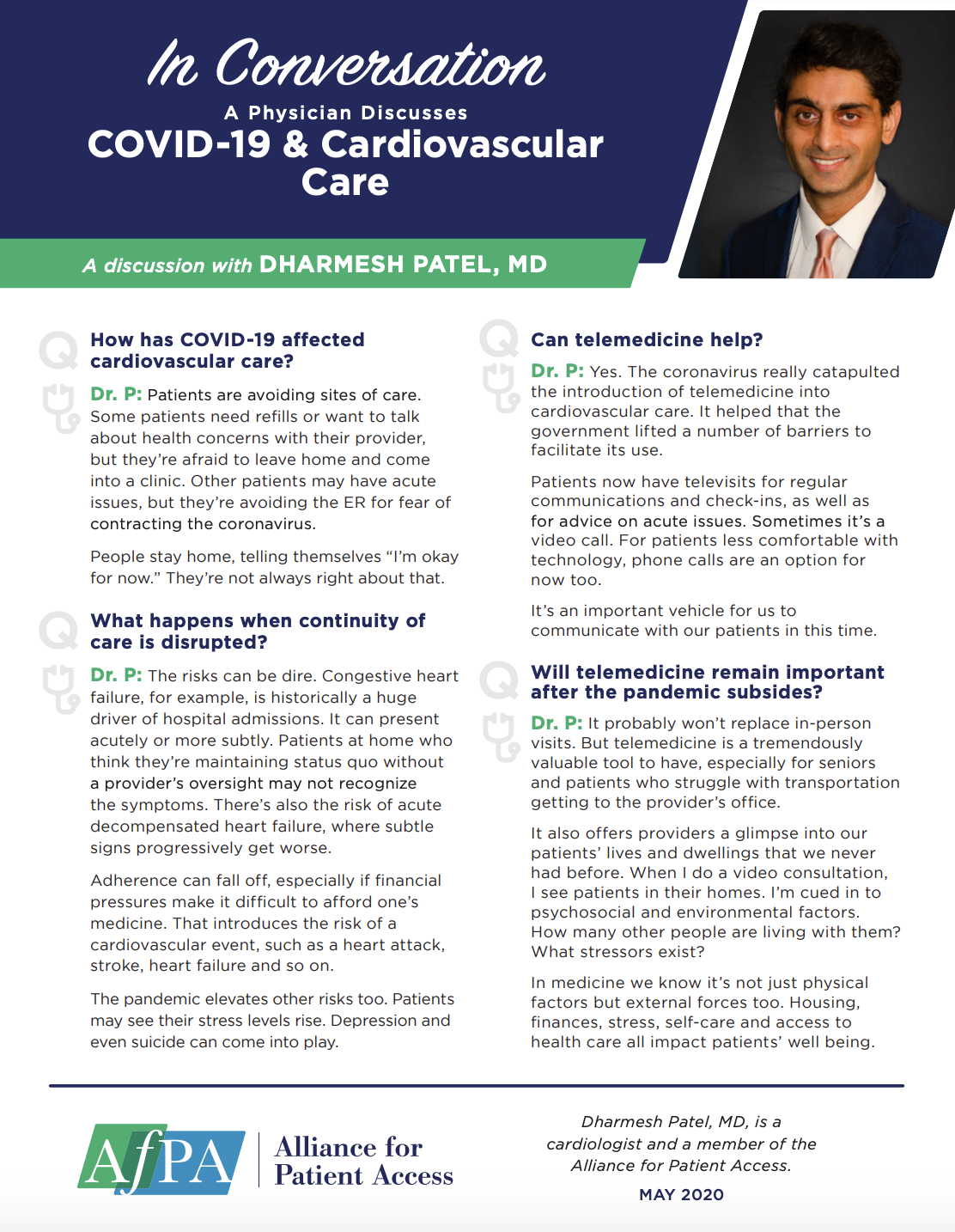
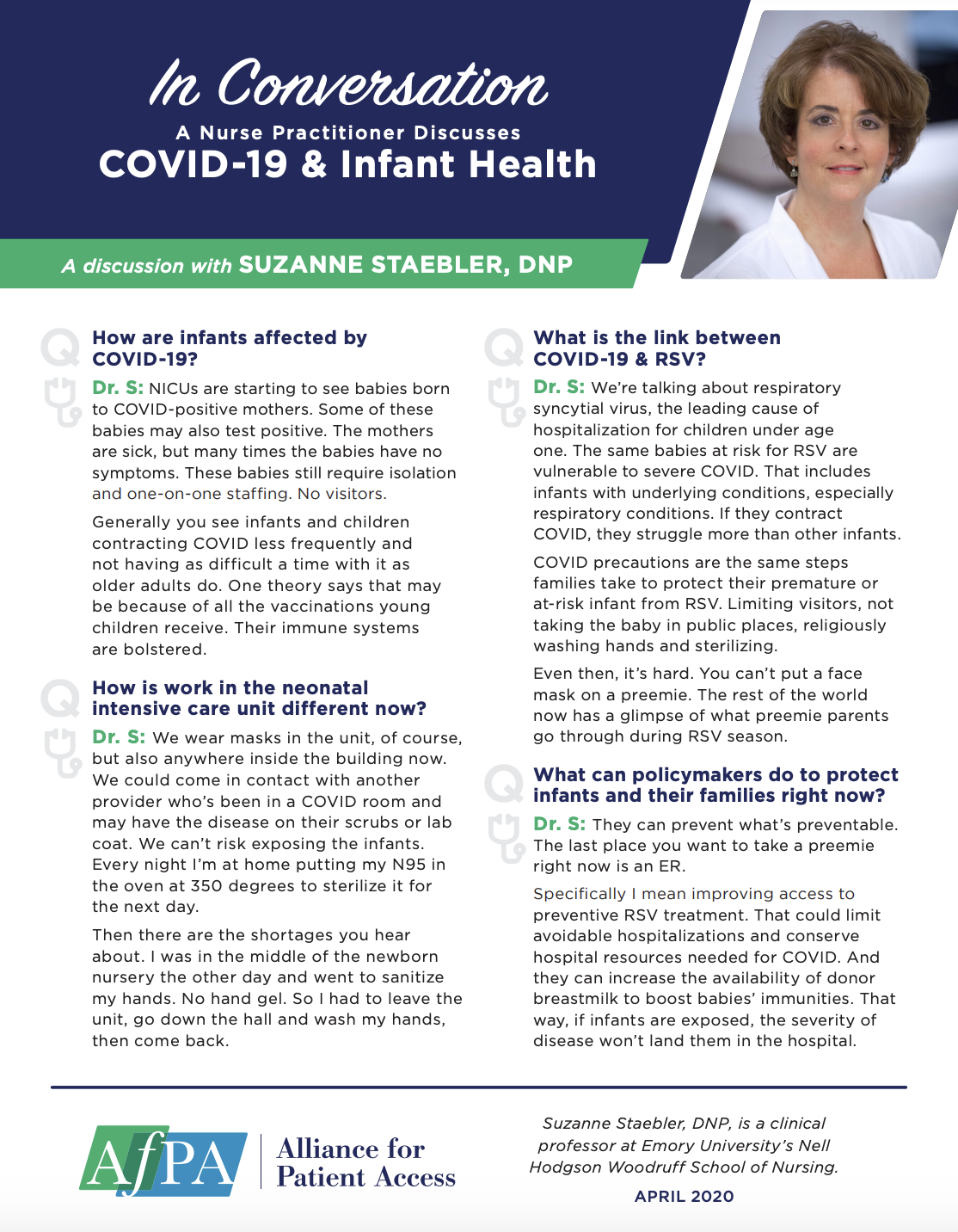
Below is a sample of the emails you can expect to receive when signed up to Alliance for Patient Access.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Data Name | Data Type | Options |
|---|---|---|
| AfPA welcomes your questions, comments, and concerns. Please fill in the form below to submit your information directly to us. Name* | ||
| Home address | ||
| City | ||
| State | ||

















































































 Arts and Entertainment
Arts and Entertainment Business and Industry
Business and Industry Computer and Electronics
Computer and Electronics Games
Games Health
Health Internet and Telecom
Internet and Telecom Shopping
Shopping Sports
Sports Travel
Travel More
More